
1 Department of Orthopedic Surgery, The University of Western Ontario, London, Ontario, Canada
2 Mechanical and Materials Engineering, The University of Western Ontario, London, Ontario, Canada
Correspondence Address
Abstract
Background : The coracoacromial ligament (CAL) is an important restraint to superior shoulder translation. The effect of CAL release on superior stability following the Latarjet is unknown; therefore, our purpose was to compare the effect of two Latarjet techniques and allograft reconstruction on superior instability.
Materials and Methods : Eight cadaveric specimens were tested on a simulator. Superior translation was monitored following an axial force in various glenohumeral rotations (neutral, internal, and external) with and without muscle loading. Three intact CAL states were tested (intact specimen, 30% glenoid bone defect, and allograft reconstruction) and two CAL deficient states (classic Latarjet (classicLAT) and congruent-arc Latarjet (congruentLAT)).
Results : In neutral without muscle loading, a significant increase in superior translation occurred with the classicLAT as compared to 30% defect (P = 0.046) and allograft conditions (P = 0.041). With muscle loading, the classicLAT (P = 0.005, 0.002) and the congruentLAT (P = 0.018, 0.021) had significantly greater superior translation compared to intact and allograft, respectively. In internal rotation, only loaded tests produced significant results; specifically, classicLAT increased translation compared to all intact CAL states (P < 0.05). In external rotation, only unloaded tests produced significant results with classicLAT and congruentLAT allowing greater translations than intact (P ≤ 0.028). For all simulations, the allograft was not significantly different than intact (P > 0.05) and no differences (P = 1.0) were found between classicLAT and congruentLAT.
Discussion: In most simulations, CAL release with the Latarjet lead to increased superior humeral translation.
Conclusion: The choice of technique for glenoid bone loss reconstruction has implications on the magnitude of superior humeral translation. This previously unknown effect requires further study to determine its clinical and kinematic outcomes.
Keywords: Coracoacromial ligament, dislocation, instability, Latarjet, shoulder, stability
Introduction
The role of the coracoacromial arch, specifically that of the coracoacromial ligament, in superior shoulder stability has been well established. [1],[2],[3],[4],[5] The majority of early reports focused primarily on the role of the coracoacromial ligament in the rotator cuff deficient shoulder. [1],[5],[6],[7] The inferior concave surface of the coracoacromial ligament acts as a static restraint, along with the acromion, to superior translation of the humeral head. Conceptually, with coracoacromial ligament resection in the setting of a large rotator cuff tear or prior surgery, the humeral head may be predisposed to anterosuperior migration, or “escape”. [7],[8] In light of this, more attention has been focused on the coracoacromial ligament to define its role in glenohumeral joint stability and kinematics.
In -vitro biomechanical studies have been performed to illustrate the role of the coracoacromial ligament in superior stability. These studies have demonstrated, but not quantified, increased superior translation following coracoacromial ligament resection with varying forces applied to the shoulder. [2],[3],[4],[7],[8] As a result, it was advocated to maintain the integrity of this structure whenever possible to avoid destabilizing the glenohumeral joint. While most studies focused on superior instability, there is also a relationship between coracoacromial ligament resection and anterior glenohumeral instability. An intact coracoacromial ligament is thought to interact with the coracohumeral ligament to provide restraint to anterior and inferior translation, as coracoacromial ligament resection has been shown to result in increased anteroinferior instability, indicating that its role in shoulder stability is larger than historically presumed. [3],[4] Post-traumatic anteroinferior glenohumeral joint instability is a common clinical entity. Frequently, shoulder dislocations result in osseous lesions, such as anterior glenoid rim fractures or Hill-Sachs impression defects, which predispose to recurrent instability. The Latarjet procedure, which involves a transfer of the coracoid along with the conjoined tendons, is an attractive surgical option for the management of anterior shoulder instability in the setting of bony defects. [9],[10] In the treatment of substantial anterior glenoid bone loss, the coracoid serves to restore the width of the glenoid to prevent further instability. [10],[11],[12],[13],[14] Additionally, the dynamic sling effect of the conjoint tendon is thought to enhance the stability provided by the bone block alone. [10] The Latarjet, as classically described, [9] involves transfer of the coracoid body with its inferior surface fixed to the anterior glenoid vault. Recently, the congruent-arc modification of the Latarjet has been described which rotates the graft 90° so its inferior surface is oriented flush with the glenoid articular surface. [13] The congruent-arc Latarjet has been reported to have a better radius of curvature match to the native glenoid, [11] better normalization of glenohumeral contact pressures, [15] and reconstitutes a greater glenoid bone defect than a coracoid oriented in the classic manner, theoretically improving anteroinferior stability. [11],[15]
The literature reports that the Latarjet coracoid transfer has been largely successful, with recurrence rates as low as 4.9% after 5 years and good to excellent patient outcomes. [12],[14] Anecdotally, it has been stated that the outcomes of the Latarjet procedure in patients older than forty five years are lower. This is theorized to be due to associated pathologies that occur in middle-aged patients, specifically disorders of the rotator cuff. The Latarjet transfer, however, does involve division of the coracoacromial ligament, which has been reported as an important structure in rotator cuff disorders. Presently, no clinical data exists demonstrating the effect of the Latarjet procedure on superior shoulder instability. Additionally, biomechanical studies investigating the Latarjet procedure have focused on anteroinferior stability, [16] while the resultant effects of superior shoulder translation remain unknown. The purpose of this in-vitro biomechanical study was to examine the effect of the Latarjet procedure and associated coracoacromial ligament resection on superior shoulder translation in an axially loaded shoulder in different static positions. We hypothesized that a structural allograft reconstruction would retain superior stability, while the Latarjet oriented in the classic manner and the congruent-arc modification would both lead to increased superior translation.
Materials and Methods
Specimen preparation
Eight fresh-frozen cadaveric forequarter specimens were used (average age seventy three years, range 69-91 years). Prior to dissection, specimen CT scans were obtained and reviewed to ensure those with pathology, such as osteoarthritis or trauma, were excluded. Specimens were prepared by transecting the humerus mid-shaft and removing attached soft tissues, while preserving the deltoid and its insertion, the rotator cuff muscles, both heads of the biceps, as well as the glenohumeral joint capsule. Image guidance was used to assist in cementing a steel-intramedullary rod fitted with a six degree of freedom (DOF) load cell (Mini45, ATI Industrial Automation, Apex, NC) [Figure 1] into the proximal shaft of the humerus. Prior to resection of the humerus, a temporary optical marker was rigidly fixed to the proximal humerus and the locations of the epicondyles were digitized. After humeral resection, the rod, which was also instrumented with an optical marker, was cemented in place while aligning it with the virtual transepicondylar axis recorded with respect to the temporary humeral marker. The distal end of the rod was then attached to the simulator via a spherical bearing that allowed four degrees of freedom, which in turn permitted full glenohumeral translation and rotation. Once attached to the simulator by the scapula pot and the spherical bearing, it was possible to manipulate the shoulder into repeatable glenohumeral orientations through adjustment of the custom stability testing apparatus [Figure 1].
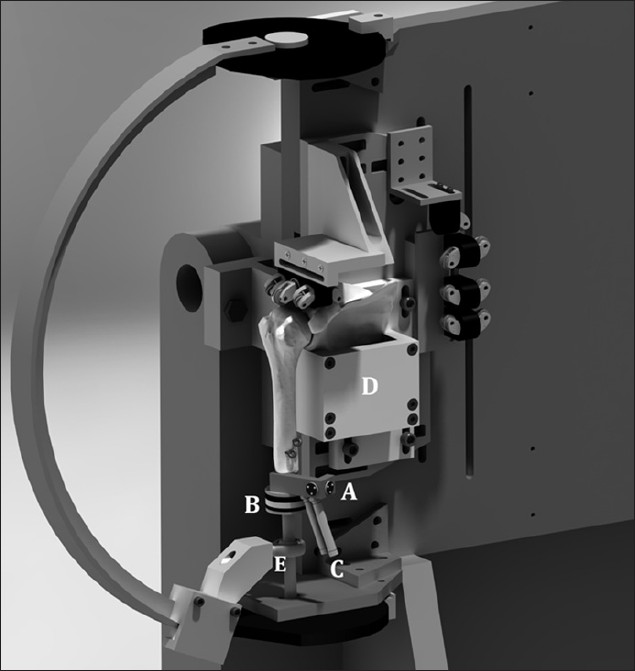 Figure 1: Computer rendering of a cadaveric shoulder specimen, with soft tissues removed for clarity, mounted to the custom shoulder stability testing apparatus in full ad duction. The apparatus is capable of independently controlling scapular elevation, and glenohumeral abduction, flexion, and humeral internal-external rotation. (A) Six degree of freedom optical tracking markers, (B) Interposed six degree of freedom humeral load cell, (C) Miniature actuators used to load long head of biceps and conjoint tendon, (D) Scapula mounting pot, (E) Spherical bearing used to connect humeral rod to apparatus without restricting glenohumeral kinematics
Figure 1: Computer rendering of a cadaveric shoulder specimen, with soft tissues removed for clarity, mounted to the custom shoulder stability testing apparatus in full ad duction. The apparatus is capable of independently controlling scapular elevation, and glenohumeral abduction, flexion, and humeral internal-external rotation. (A) Six degree of freedom optical tracking markers, (B) Interposed six degree of freedom humeral load cell, (C) Miniature actuators used to load long head of biceps and conjoint tendon, (D) Scapula mounting pot, (E) Spherical bearing used to connect humeral rod to apparatus without restricting glenohumeral kinematics
The in vitro shoulder simulator allowed unconstrained glenohumeral motion [Figure 1]. Simulated loads were applied to eight shoulder muscle groups (three heads of the deltoid, supraspinatus, infraspinatus and teres minor, subscapularis, long head of biceps and the conjoined group) after passing sutures (#5 Ethibond, Ethicon, Somerville, NJ) through their musculotendinous junctions. Conjoint tendon and long head of biceps loading were achieved by suturing the tendons and passing the sutures through eyelets placed on the humerus that replicated the muscles’ natural lines of action. Sutures were connected to two miniature pneumatic actuators mounted on the humerus. The conjoint tendon was loaded with 10 N based on a previous study assessing conjoined tendon loading. [17] The supraspinatus, subscapularis, and the combination of the infraspinatus and teres minor were all loaded with 7.5 N each. The anterior, lateral and posterior heads of the deltoid were each loaded with 5 N. [18],[19],[20],[21] Optical markers (Optotrak Certus, NDI, Waterloo, ON) were mounted on the scapula and humerus, and digitizations were made in order to create an Euler rotation sequence consistent with ISB standards. [22] Specifically, digitizations of the inferior angle, root of the spine, and the posterolateral aspect of the acromion were made on the scapula and used to create a scapular coordinate system. On the humerus, the previous medial and lateral epicondylar digitizations were used in addition to the center of the humeral head, which was determined from kinematic recordings, to construct a humeral coordinate system. [23],[24],[25]
Testing protocol
The protocol was designed to test the effect of coracoacromial ligament resection, following classic and congruent-arc Latarjet procedures, on superior shoulder translation in an axially loaded specimen with and without simulated muscle loads. Repetitive access to the glenohumeral joint was required in keeping with the repeated measures design of the study. In order to allow this without compromising stability with subsequent tests, access was gained via an extended lesser tuberosity osteotomy. The osteotomy was then fixed using two bicortical 1/8″ nut-and-bolt constructs to ensure rigid fixation after each exposure. Previous studies have found that shoulder stability and range of motion have not been significantly affected with this technique. [20] Once the joint was accessed, points were digitized on the glenoid and were used to create a co-ordinate system for assessing humeral head translations.
Five conditions were tested for each specimen in this protocol: Intact specimen, 30% anterior glenoid bone defect, allograft coracoid reconstruction, classic Latarjet procedure, and the congruent-arc modification of the Latarjet. After the intact specimen was tested, a 30% anterior glenoid bone defect was created following the protocol detailed by Yamamoto et al. [26] Reference was made to the work of Saito et al. who demonstrated that a typical defect associated with anterior shoulder instability can be found in the 3:01 o’clock position on the glenoid. [27] Calipers were used to identify a 30% glenoid segment starting from the anterior rim, which was then resected with a microsagittal saw.
After testing the 30% anterior glenoid bony defect, an allograft coracoid was affixed to the anterior aspect of the glenoid in the region of the previously created defect [Figure 2]a. The allograft coracoid specimens used were size- and side-matched to ensure appropriate fit. The preparation and orientation of the graft was similar to that described for the classic Latarjet procedure. [9],[28] The graft was secured to the glenoid with two 3.5 mm cortical screws.
After testing the allograft specimen, classic or congruent-arc Latarjet procedures were performed in a randomized fashion. [9],[28] The coracoid body was exposed and osteotomized at its angle. The attached conjoint tendon was transferred with the coracoid to the anterior glenoid, passed through a subscapularis split and loaded via an actuator on the humeral shaft. For the classic technique, the inferior surface of the coracoid was fixed to the glenoid with two 3.5 mm cortical screws [Figure 2]b. The congruent-arc technique was performed as described by De Beer et al. [13] with rotation of the graft 90° so that the inferior surface would sit flush with the glenoid articular surface [Figure 2]c. For each state, specimens were tested with and without a load applied to the rotator cuff, conjoint tendon, long head of biceps and anterior, lateral and posterior heads of the deltoid.
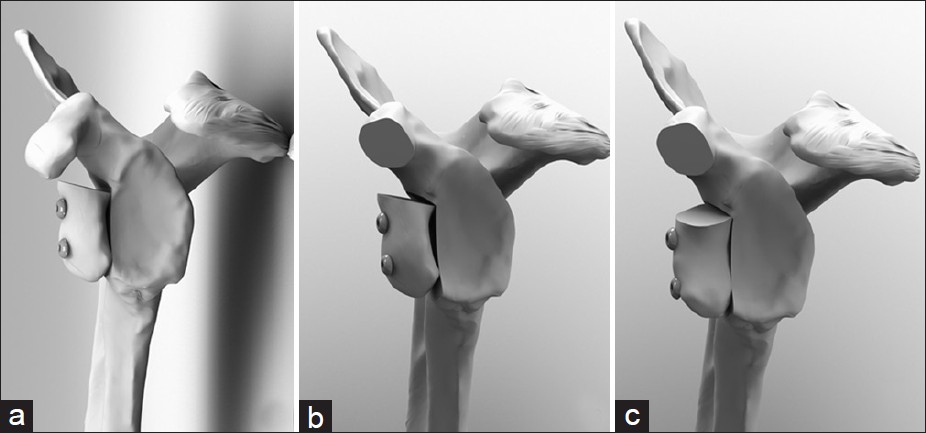 Figure 2: Coracoid reconstructions of a 30% anterior glenoid defect on a left specimen. (a) Allograft coracoid reconstruction, (b) Classic Latarjet coracoid transfer, (c) Congruent-Arc Latarjet coracoid transfer. Note that in each rendering, all soft tissues are omitted for clarity. Also, in the case of the allograft reconstruction the coracoacromial ligament is preserved
Figure 2: Coracoid reconstructions of a 30% anterior glenoid defect on a left specimen. (a) Allograft coracoid reconstruction, (b) Classic Latarjet coracoid transfer, (c) Congruent-Arc Latarjet coracoid transfer. Note that in each rendering, all soft tissues are omitted for clarity. Also, in the case of the allograft reconstruction the coracoacromial ligament is preserved
Stability testing
Superior joint stability was tested in three configurations: (1) Neutral rotation (2) Internal rotation and (3) External rotation all in 0 degrees of flexion, and 0 degrees of abduction. The positions of internal and external rotation were established by rotating the humerus until a pre-defined torque of ± 0.8 Nm was achieved. This magnitude was set based on repeated clinical examinations of a pilot specimen by an orthopedic surgeon (XXX) until meeting resistance consistent with routine clinical examination, measuring on average 0.8 Nm.
Superior glenohumeral joint stability was measured by determining superior humeral head translation while applying a quasi-static axial load up to 80 N. The magnitude of humeral head translation was defined as the maximum point of displacement along the y-axis, measured in millimeters, following a maximum applied force of 80 N. Two loading cycles were applied to the specimens in each particular condition and position. The six degree of freedom humeral load cell was used for real-time feedback and to record the applied load, while joint kinematics were quantified using the optical tracking markers.
Statistical analysis
Statistical analyses were conducted with a statistical package (SPSS Inc., Chicago, IL), using a combination of one-way repeated measures Analyses of Variance (ANOVAs) and pairwise comparisons. Each analysis consisted of five levels: Intact, 30% glenoid bone defect, allograft coracoid, and the classic and congruent arc Latarjet procedures. Significance was set at P < 0.05.
Results
Humeral head translation: Neutral rotation
In the neutral position without muscle loading, a statistically significant increase in superior translation was noted with the classic Latarjet procedure as compared to the 30% anterior glenoid bone defect (3.4 mm ± 2.3, P = 0.046) and the allograft reconstruction (3.1 mm ± 2.1, P = 0.041). The congruent-arc Latarjet did not result in significant greater superior translation (P > 0.05) and the allograft reconstruction was not significantly different than the intact condition (P = 1.0).
After activation and loading of the shoulder girdle muscles, the overall magnitude of translation decreased in all conditions, however, superior translation after the classic Latarjet was significantly greater than the intact state (1.2 mm ± 0.6, P = 0.005) and the allograft reconstruction (0.9 mm ± 0.4, P = 0.002). Similarly, during active muscle loading the congruent arc Latarjet was also found to have significantly greater superior translation compared to both the intact condition (1.5 mm ± 0.9, P = 0.018) and the allograft reconstruction (1.2 mm ± 0.7, P = 0.021). The allograft reconstruction, however, was not significantly different than the intact condition (P = 1.0). Additionally, no significant differences (P = 1.0) were found between the classic and the congruent-arc Latarjet conditions with respect to superior translation in neutral rotation, with or without muscle loading [Figure 3].
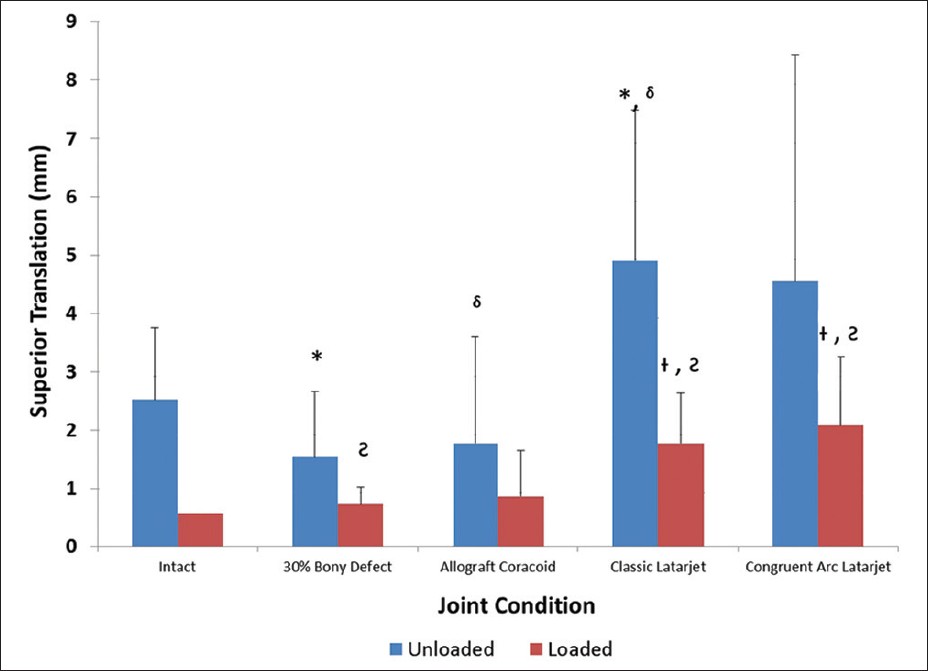
Figure 3: Superior humeral head translation data in adduction, neutral rotation
Humeral head translation: Internal rotation
In glenohumeral internal rotation without muscle loading, there were no significant increases in humeral head superior translation between the conditions (P > 0.05). With physiologic loads applied to the muscle groups, the overall magnitudes of translation decreased. However, a significant increase in superior translation occurred after the classic Latarjet as compared to the intact (1.7 mm ± 1.1, P = 0.041), 30% bone defect (1.5 mm ± 0.9, P = 0.022) and the allograft (1.3 mm ± 0.9, P = 0.037). In contrast, the congruent arc Latarjet was not found to be significantly different from any other condition (P > 0.078). No significant differences were noted between the allograft reconstruction and the intact condition (P = 1.0). Additionally, no significant differences ( P = 1.0) were found between the classic and the congruent-arc Latarjet procedures with respect to superior translation in internal rotation, with or without muscle loading [Figure 4].
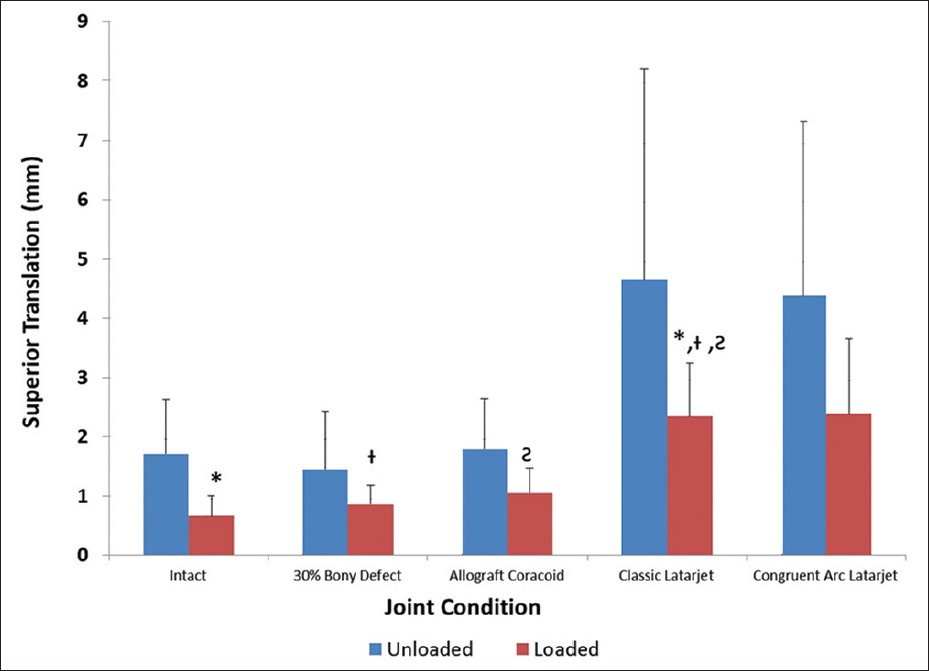
Figure 4: Superior humeral head translation in adduction, internal rotation
Humeral head translation: External rotation
In external rotation without muscle loading, the classic and the congruent-arc Latarjet procedures were found to have significantly greater superior humeral head translation as compared to the intact condition (3.2 mm ± 2.0, P = 0.028 and 2.6 mm ± 1.5, P = 0.017, respectively), while the allograft reconstruction was not significantly different from intact (1.1 mm ± 1.7, P = 0.991).
With the application of physiologic muscle loading, no significant differences were identified between the conditions ( P > 0.05). Additionally, no significant differences (P = 1.0) were found between the classic and the congruent-arc Latarjet procedures with respect to superior translation in external rotation, with or without muscle loading [Figure 5].
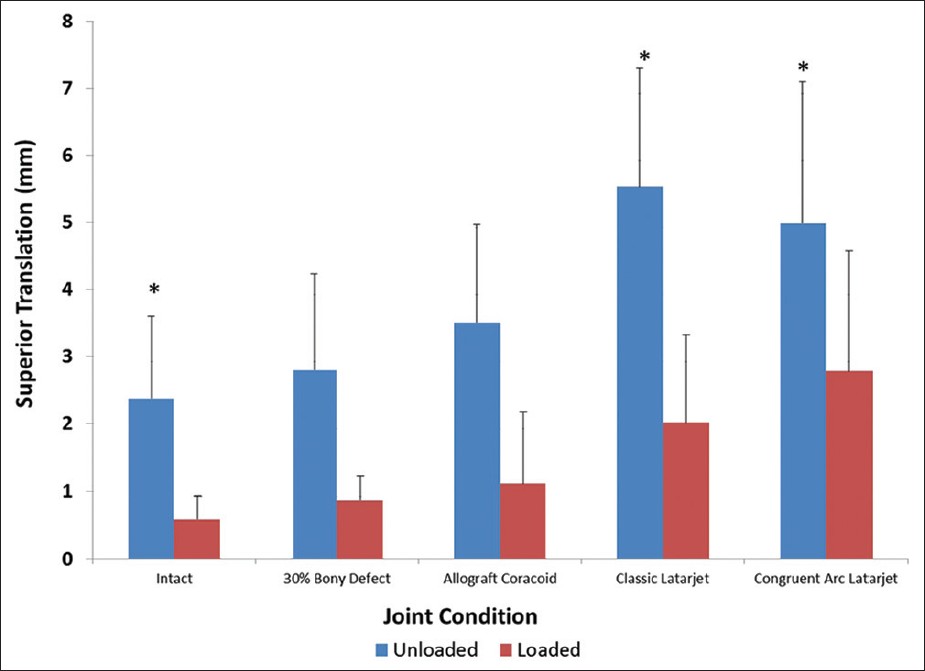
Figure 5: Superior humeral head translation in adduction, external rotation
Humeral head translation: Load effect
In all positions, across all conditions, applying physiologic muscle loading to the rotator cuff, the long head of biceps, the conjoined tendon, and the deltoid muscle reduced the overall magnitude of superior displacement. In the unloaded neutral position, testing produced the largest magnitude of superior translation with a maximum mean of 5.0 mm (±2.6 mm), which occurred after the classic Latarjet. Applying a simulated load reduced this value to 1.8 mm (±0.9 mm) of displacement.
In internal rotation, maximum translation with the unloaded muscle groups was seen in the classic Latarjet condition as well, with an average superior translation of 4.7 mm (±3.5 mm). Applying a load in this position reduced the average translation to a maximum of 2.4 mm (±0.9 mm).
In external rotation in the unloaded state, the maximum average superior translation was measured at 5.6 mm (±1.8 mm) once again in the classic Latarjet condition, while loading the cuff reduced maximum translation to 2.1 mm (±1.3 mm).
Discussion
The effect of coracoacromial ligament resection on superior shoulder translation has been demonstrated in several biomechanical studies; however, these have largely focused on the effect in rotator cuff-deficient shoulders or those with symptoms of impingement. [1],[2],[3],[5],[7] To date, no study has investigated the effect of coracoacromial ligament resection in patients with anteroinferior instability undergoing a stabilizing Latarjet coracoid transfer procedure. Our results indicate that performing a Latarjet procedure can lead to an increase in superior shoulder translation in most joint configurations and loading conditions. This highlights the importance of the coracoacromial ligament as a restraint to superior humeral head translation, even in cases with an intact rotator cuff. Additionally, we compared the Latarjet procedures with allograft reconstruction and found that the allograft did not significantly differ from the intact condition for the parameters examined. The clinical significance of these findings is not definitely known. We believe that completely understanding the biomechanics of the Latarjet procedure, especially in older patients, may help identify patient sub-groups that may be better served with alternative reconstructive procedures.
In our model, the application of physiologic muscle loads dampened the abnormal superior displacement values after the Latarjet procedures. This reduction in the overall magnitude of superior translation was evident across all states and in all tested positions. This likely relates to the static stabilizing features of a concentrically reduced loaded glenohumeral joint, and the dynamic stabilizing effect of the tensioned rotator cuff muscles. [29],[30],[31] This knowledge of the important stabilizing effects of the rotator cuff muscles reaffirms the importance of post-operative muscle strengthening protocols, which may be especially important after a Latarjet procedure.
Glenohumeral joint positioning had substantial effects on the magnitude of superior humeral head translation. While only slight differences in superior translation were present in the neutral position, marked significant differences were noted in the internal and external rotation positions between the different loading cycles. In the internally rotated position, no significant differences were found in the unloaded group between the various states; however, physiologic muscle loading resulted in significant increases in superior translation in the classic Latarjet group as compared to all states with an intact coracoacromial ligament. Perhaps muscle loading and terminal rotation allows the physiologic restraints of the specific ligamentous stabilizers to function at their correct length and tension, [32] and resection of key stabilizing structures in this condition will exemplify their role in superior stability.
In external rotation, the unloaded states demonstrated significantly increased superior translation in the classic and congruent-arc Latarjet groups as compared to intact ( P = 0.028, 0.017). Applying physiologic muscle loads, however, resulted in no significant differences in superior translation for either state. This may relate to the natural posterosuperior translation that occurs in the loaded, externally rotated shoulder, perhaps negating the importance of the coracoacromial ligament as significant translations may be reduced by the tensioned anterior glenohumeral ligaments. [29],[30]
In addition to testing the effects of the Latarjet procedures on superior translation, we also tested a structural allograft reconstruction condition with an intact coracoacromial ligament. For the allograft, we chose an allograft coracoid oriented in the classic Latarjet manner that was contoured to sit flush with the glenoid articular surface. Testing of the allograft demonstrated that there were no significant differences in superior translations between it and the intact condition in any scenario tested (P > 0.05). The obvious benefit of the allograft procedure is that it allows preservation of the native coracoacromial arch, presumably decreasing any superior translation that would arise due to coracoacromial ligament disruption. The use of allograft, however, is not without potential risks, such as graft resorption, disease transmission, cost and prominent intra-articular hardware.
Clinical studies have reported that the average acromiohumeral distance measures between 10-15 mm in healthy individuals and 7 mm in patients with large rotator cuff tears. [33] The greatest magnitudes of superior translation in the present study occurred with the classic Latarjet procedure without loading with a mean of 5.6 mm, while with loading the maximum mean dropped to 2.1 mm. With physiologic muscle loading, the overall mean superior translation with the Latarjet procedures was 2.3 mm. Although the values for superior translation following the Latarjet were usually found to be statistically significant, it is unknown whether they are clinically significant. Further studies are needed to determine the manifestations of superior shoulder translation following Latarjet coracoid transfer to determine if the allograft procedure has a potentially beneficial role by maintaining superior stability. [33] Although the allograft reconstruction may maintain superior stability, it lacks the sling effect of the conjoint tendon transfer of the Laterjet, which is theorized to provide additional dynamic stability to the glenohumeral joint. [16] Careful patient selection for the utilization of one particular surgical procedure over another is required. For example, older patients with recurrent instability, glenoid bone loss and rotator cuff disease, may be found to do better with structural glenoid bone grafting over a Latarjet procedure.
The congruent-arc modification of the Latarjet, which rotates the coracoid graft 90° relative to the classic Latarjet procedure, has several purported advantages including a matching radius of curvature to the glenoid and the ability to reconstitute greater glenoid bone loss. Due to the matching radius of curvature and the potential for greater bony conformity and constraint, it is conceivable that the coracoid oriented in the congruent manner could decrease superior humeral head translation. Our results, however, indicate that there were no significant differences (P > 0.05) between the congruent-arc modification and the classic Latarjet with regard to superior translation.
Limitations of this study are consistent with those of other cadaveric studies, including the use of elder donor specimens. Additionally, the findings reported represent time-zero effects for specific joint configurations and load conditions, and thus it is not possible to extrapolate long-term outcomes or effects of other joint conditions.
Conclusion
The classic and congruent-arc Latarjet procedures, which disrupt the coracoacromial ligament, increase superior humeral head translation. Superior translation after glenoid reconstruction with a structural allograft, however, is not substantially different from the intact condition. Further clinical studies are required to elucidate the implications of increased superior translation due to the Latarjet reconstruction.