
1 School of Physical Therapy, University of Western Ontario, London, Ontario, Canada
2 Co-Director, Clinical Research Lab, Hand and Upper Limb Centre, St Joseph’s Health Centre, London; Professor, School of Rehabilitation, McMaster University, Hamilton, Ontario, Canada
3 School of Rehabilitation Sciences, McMaster University, Hamilton, Ontario, Canada
4 Department of Mechanical and Materials Engineering, University of Western Ontario; Co-Director, Wolf Orthopaedic Biomechanics Lab, Fowler Kennedy Sport Medicine Clinic, London, Ontario, Canada
5 Co-Director, Wolf Orthopaedic Biomechanics Lab, Fowler Kennedy Sport Medicine Clinic; School of Physical Therapy, University of Western Ontario, London, Ontario, Canada
6 Hand and Upper Limb Centre, St Joseph’s Health Centre, London, Ontario, Canada
Correspondence Address
Abstract
Purpose: Video-based movement analysis software (Dartfish) has potential for clinical applications for understanding shoulder motion if functional measures can be reliably obtained. The primary purpose of this study was to describe the functional range of motion (ROM) of the shoulder used to perform a subset of functional tasks. A second purpose was to assess the reliability of functional ROM measurements obtained by different raters using Dartfish software.
Materials and Methods: Ten healthy participants, mean age 29 ± 5 years, were videotaped while performing five tasks selected from the Disabilities of the Arm, Shoulder and Hand (DASH). Video cameras and markers were used to obtain video images suitable for analysis in Dartfish software. Three repetitions of each task were performed. Shoulder movements from all three repetitions were analyzed using Dartfish software. The tracking tool of the Dartfish software was used to obtain shoulder joint angles and arcs of motion. Test-retest and inter-rater reliability of the measurements were evaluated using intraclass correlation coefficients (ICC).
Results: Maximum (coronal plane) abduction (118° ± 16°) and (sagittal plane) flexion (111° ± 15°) was observed during ‘washing one’s hair;’ maximum extension (−68° ± 9°) was identified during ‘washing one’s own back.’ Minimum shoulder ROM was observed during ‘opening a tight jar’ (33° ± 13° abduction and 13° ± 19° flexion). Test-retest reliability (ICC = 0.45 to 0.94) suggests high inter-individual task variability, and inter-rater reliability (ICC = 0.68 to 1.00) showed moderate to excellent agreement.
Conclusion: Key findings include: 1) functional shoulder ROM identified in this study compared to similar studies; 2) healthy individuals require less than full ROM when performing five common ADL tasks 3) high participant variability was observed during performance of the five ADL tasks; and 4) Dartfish software provides a clinically relevant tool to analyze shoulder function.
Keywords: Dartfish, DASH, functional range of motion, reliability, shoulder
Introduction
Shoulder movement is important for performing activities of daily living (ADLs), including household chores, preparing meals, and recreational activities. Shoulder dysfunction can cause reduced mobility leading to decreased functional independence and a decreased quality of life. [1],[2],[3] Optimizing shoulder range of motion (ROM) to facilitate ADL performance is an important goal for surgeons and clinicians who treat individuals with shoulder dysfunction.
Several studies [4],[5],[6],[7],[8],[9],[10],[11] have investigated the shoulder-specific motions required for ADLs. These studies have employed a variety of measurement techniques, ranging from the standard goniometry to three-dimensional motion analysis systems. [4],[5],[6],[7],[8],[9],[10],[11] Each technique has its own inherent challenges in measuring functional motion, largely due to the complexity of the shoulder joint. Movement analyses of the upper body using three-dimensional motion analysis systems have focused on the plane of elevation, angle of elevation, and angle of rotation of the shoulder. [4] Although this method accurately defines the axes of movement and facilitates visualization of the movements, [4] clinically, shoulder ROM is measured and documented in planes of movement such as flexion/extension, abduction/adduction, and internal/external rotation. Goniometry is used in clinical practice but is not designed to test complex, dynamic movements. Exploring alternate, feasible methods to measure range of movement during activity can provide greater insight into shoulder function, which can translate into improved recovery from shoulder impairments. Video-based motion analysis is an approach being introduced into clinical practice to evaluate kinematic changes in movements corresponding to treatment. Dartfish is an example of software that is ideally suited to motion analysis and provides contextually relevant feedback to monitor and evaluate patients’ treatment progress in clinical settings. The software permits analysis of video inputs from a variety of sources and provides kinematic outputs to facilitate spatial and temporal analysis of movement. Dartfish has been used to assess individuals’ performance during complex functional tasks (i.e., walking, lifting) [12],[13],[14],[15] and during sport performance (i.e., speed walking, sprinting). [16],[17],[18] Moreover, Dartfish has been established as a valid and reliable tool to measure lower body (i.e., hip, knee) [13] and upper limb (i.e., shoulder) movements. [12] Dartfish has capability to identify various movement parameters including x, y spatial coordinates, range of movement, velocity, amplitude, frequency, and movement time from video inputs associated with task performance. This creates a movement analysis approach that is financially feasible [12] and can be implemented in a variety of contexts including clinical applications, to identify changes in movement and corresponding improvements in task performance. For example, it is possible to use the Dartfish app tool to provide immediate, in-clinic visual feedback to patients on shoulder mechanics pre- and post-surgical intervention. The visual information is readily imported into Dartfish software from which reports can be prepared with pictures and video providing visual and written feedback that can be used to target treatment approaches. A targeted treatment approach will expedite recovery and facilitate individuals’ return to normal function following shoulder impairment.
Although Dartfish has promising applications in clinical and research, technical precision may be less than expected of traditional motion analysis laboratories. Conversely, if this method has acceptable levels of precision/reliability, it would allow clinicians and clinical researchers to collect additional data on dynamic shoulder motion. The ability to collect data in clinically or applied research contexts may outweigh the challenges in using video-based movement analysis. Therefore, it is important to establish the reliability and validity of this technique for movement analysis while performing functional tasks. Identifying the measurement properties of Dartfish while determining shoulder mechanics associated with a commonly used patient-reported outcome measure (PROM) is one approach to link the clinical utility of Dartfish with a current standard of practice for assessing the impact of shoulder impairment on individuals’ function. The Disabilities of the Arm, Shoulder and Hand questionnaire (DASH) is frequently used to assess patient’s perceptions of upper extremity function. [20] The DASH [20],[21] samples a variety of ADL tasks that are considered relevant to many individuals at risk with upper extremity pathology. Selecting ADL tasks based on the DASH provides a structure for reducing the potential pool of tasks assessed, and provides an opportunity to better understand which DASH items might be most salient to patients with shoulder pathology. Hence, the specific aims of this study were to (1) identify the movement requirements of five ADLs selected from the DASH and (2) assess the test-retest and inter-rater reliability of measurements of shoulder ROM obtained using Dartfish motion-analysis software.
Materials and Methods
Participants
Ten healthy participants, aged 18 years and above, without any shoulder complaints participated in the study. Western University’s Research Ethics Board approved the study protocol, and all participants provided informed, written consent prior to study participation. Participants were excluded if they had any history of pain, trauma, shoulder dysfunction, current medical disease, neurological or cardiovascular diseases. There were equal numbers of males and females in the study. The mean age was 29 ± 5 years, and mean height was 173.2 cm ± 8.6 cm. The testing was performed on the dominant hand. Hand dominance was self-reported by the participants. Eight participants were right-hand dominant, and two participants reported left-hand dominance.
Data collection
DASH – activity of daily living (ADL) tasks
Five ADL tasks were selected from the DASH to represent a spectrum of ADLS and included:
- Opening a tight jar,
- Pushing a heavy door,
- Changing an overhead bulb,
- Washing one’s hair, and
- Washing one’s back. Participants were instructed to perform these tasks in their usual manner, and the tools used to typically perform these tasks (i.e., a light bulb) were provided.th
Equipment set-up and procedure
Two commercially available video cameras were used for this study: A Panasonic® HDC-SD60 (high definition camera) and Panasonic® PV-GS320 (standard definition) camera. The cameras were positioned as follows: The standard definition camera was placed facing the participants’ dominant hand side (to record the activities performed in the sagittal plane), and the high definition camera was placed behind and facing the same direction as the participant (to record the activities performed in the coronal plane). The position of the cameras was standardized for all participants. The experimental set-up is shown in [Figure 1].
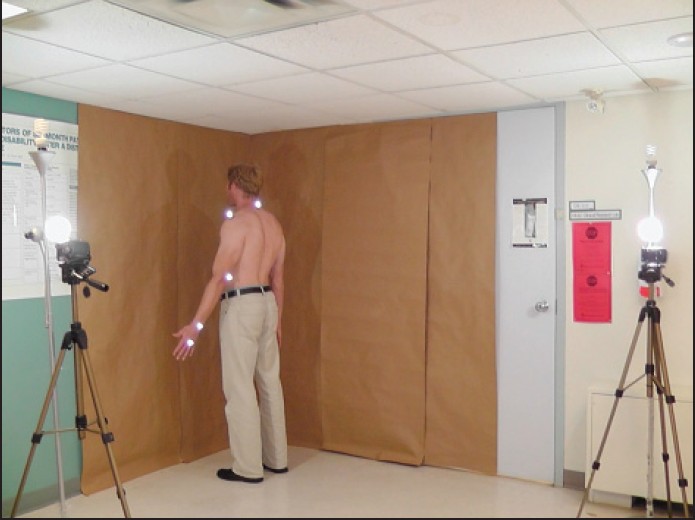
Figure 1: View of the experiment set-up. The subject is in the starting position with markers applied
Five reflective markers were placed at anatomic landmarks commonly used by clinicians as points of reference when determining changes in joint motion. The anatomic landmarks were located, and reflective markers were affixed with adhesive tape by one of the two raters. The five markers were placed on the side of the subject’s dominant arm at the following locations: C7 spinous process, acromion superiorly, midway between the medial and lateral humeral epicondyles posteriorly, midway between the radial and ulnar styloid processes dorsally, and on the head of the third metacarpal. For the purpose of this study, we were interested in positional outputs associated with markers located at the acromion and the lateral humeral epicondyle. Data from the remaining markers allow the possibility of future studies to determine hand and wrist mechanics in ADLs.
The procedures for performing the five ADLs selected from the DASH were standardized and demonstrated to all the subjects to ensure visibility of the markers throughout the performance of the activities. The start and end position for all activities was in a standing, anatomically neutral position [Figure 2]a and b. During the jar-opening task, it was necessary that the participants perform the task laterally from the anatomical neutral position to facilitate visibility of the makers in both sagittal and coronal planes. All participants were asked to perform the five ADL DASH tasks from the anatomical neutral position (except the jar opening task) and were instructed to perform these activities using natural movements. The participants were requested to perform the five ADL tasks three consecutive times before moving to the next task.
 Figure 2: The coordinate system defined by the Dartfish is shown the figure (a) The coordinate system for left hand dominant study participant (b) The coordinate system for right hand dominant study participant
Figure 2: The coordinate system defined by the Dartfish is shown the figure (a) The coordinate system for left hand dominant study participant (b) The coordinate system for right hand dominant study participant
Data analysis
Shoulder movement analysis using Dartfish
Participants were recorded using the two video cameras while performing each of the five DASH tasks. The video images were imported into Dartfish ProSuite 5.5 video software and were edited into short video clips of the participants performing each of the 5 ADL DASH tasks. Two raters analyzed each of these clips using the angle-tracking feature of the Dartfish software. The process of using the angle-tracking feature was standardized between the two raters. The two raters were unaware of each other’s results.
The angle-tracking feature of the Dartfish software identified angles of movement and arcs of motion throughout the performance of the ADL tasks. An angle of movement was defined as the angle created when two lines extended through the marker at the point of rotation. Arc of motion was determined as the difference between the maximum and minimum angle of movement during task performance. The angle-tracking feature followed the reflective makers placed on anatomic landmarks throughout performance of the five ADL tasks to determine the angles of movement. Occasionally, the automatic tracking of the reflective markers was lost. When this occurred, the tracking was performed manually. The position of these markers throughout the performance of the task was obtained in the form of x, y coordinates. The Dartfish software tracked the markers and reported their positions at a rate of 30 frames per second.
Maximum and minimum shoulder angles of movement and arc of motion were identified for each participant during each task. The angles of movement and arc of motion data were transferred to Microsoft® Office Excel 2007 and SPSS 17 statistical analysis software, which was used for analyses.
Thoracohumeral angle
Functional movements occur as a combination of movements. For example, a simple activity of pushing a heavy door occurs as a combination of flexion and abduction. Functional activities do not occur in a single plane. Thus, thoracohumeral angle was determined as the best way to report the shoulder angles of movement to provide clinically meaningful data. A similar concept is used for ROM measurement using a standard goniometer. [22],[23] The thoracohumeral angle in degrees was defined by connecting a vertical-plumb line from the acromion to approximately the greater trochanter with a second line from the acromion to the lateral humeral epicondyle. Thoracohumeral angles were identified in the sagittal and coronal planes. The thoracohumeral angle measured from the sagittal plane represented flexion/extension, whereas the thoracohumeral angle measured from the coronal plane represented abduction/adduction. A positive thoracohumeral angle value in the sagittal and coronal planes represented flexion and abduction, respectively. Correspondingly, negative thoracohumeral angles in the sagittal and coronal and sagittal planes represented extension and adduction, respectively.
The thoracohumeral angle in the coronal and sagittal planes were plotted against time in seconds to graphically represent the movement patterns required for completion of each task [Figure 3]. Plotting the mean trajectory of the angles produced for all individual activities was not possible, as time required for the completion of a particular activity was not standardized. Hence, to calculate the mean trajectory of the angles, data were converted to percent completion from the time required to complete the activity with the assumption that participants completed tasks at a constant velocity. By converting the data into percent completion, the data were standardized.
 Figure 3: Thoracohumeral angle in the coronal and sagittal planes for all subjects plotted against time (in seconds) during performance of activity as follows: (a) Pushing a heavy door, (b) Changing an overhead light bulb, (c) Opening a tight jar, (d) Washing one’s back, and (e) Washing one’s hair
Figure 3: Thoracohumeral angle in the coronal and sagittal planes for all subjects plotted against time (in seconds) during performance of activity as follows: (a) Pushing a heavy door, (b) Changing an overhead light bulb, (c) Opening a tight jar, (d) Washing one’s back, and (e) Washing one’s hair
Finally, to obtain thoracohumeral angles of movement at common percent completion intervals, data interpolation technique was used. This processed data was used to plot the mean trajectory graphs of thoracohumeral angles in the coronal plane against thoracohumeral angles in the sagittal plane for all five DASH tasks [Figure 4]a-d.
 Figure 4: Thoracohumeral angle in the coronal plane against the thoracohumeral angle in the sagittal planes during performance of activity as follows: (a) Pushing a heavy door, (b) Changing an overhead light bulb, (c) Opening a tight jar, (d) Washing one’s back. and (e) Washing one’s hair
Figure 4: Thoracohumeral angle in the coronal plane against the thoracohumeral angle in the sagittal planes during performance of activity as follows: (a) Pushing a heavy door, (b) Changing an overhead light bulb, (c) Opening a tight jar, (d) Washing one’s back. and (e) Washing one’s hair
Reliability analysis
Statistical analysis for inter-rater reliability was performed using SPSS 17 statistical software package for Microsoft Windows® (SPSS Inc., Chicago, IL, USA). An intraclass correlation coefficient (ICC) (two-way random model with consistency) was used to assess the test-retest reliability between the three trials [24]. An ICC (two-way random model with absolute agreement) was used to assess inter-reliability between the mean scores of three trials measured by the two raters. This model was selected to account for any systematic errors between the two raters. For interpretation of the reliability, an ICC value of less than 0.40 was considered poor agreement, between 0.40 and 0.75 was considered moderate agreement, and above 0.75 was considered excellent agreement. [24],[25]
Standard error of measurement (SEM) was calculated using the formula SEM analyses were performed based on the ICC value of inter-rater reliability, as it was also based on the mean angles of the three trials.
Results
Shoulder movement analysis using Dartfish
The maximum and minimum angles and arc of motion for all DASH activities are illustrated in [Table 1]. These results identified the maximum, functional thoracohumeral angle required to perform the five selected DASH tasks is 118° ± 16°, 95% CIs (108°,128°) in sagittal plane flexion (washing hair – maximum angle), 112° ± 14°, 95% CIs (102°,121°) in coronal plane abduction (washing hair – maximum value), and −67° ± 9°, 95% CI’s (−74°, −62°) (washing back) in sagittal plane extension.
 Table 1: Thoracohumeral angle in both planes (coronal and sagittal) for all subjects (n = 10)
Table 1: Thoracohumeral angle in both planes (coronal and sagittal) for all subjects (n = 10)
The movement patterns of all subjects for the individual activities plotted against the time for completion are shown in [Figure 3]; these demonstrated substantial variations in the movement patterns between subjects during the performance of the same activity.
The mean trajectory of thoracohumeral angles produced for all individual activities are shown in [Figure 4]. The subjects were positioned with their arm in slight thoracohumeral elevation in the coronal plane or abduction (6° to 8°) and negative thoracohumeral elevation in the sagittal plane or extension (−5° to −12°) in the starting and ending positions. The thoracohumeral angles in both planes increased gradually, and peak joint angles were reached during performance of the task.
Reliability analysis
0The majority of ICCs indicate moderate to excellent agreement within and between raters. The ICC values of test-retest reliability ranged from 0.45 to 0.94 [Table 2]. The ICC values of inter-rater reliability ranged from 0.68 to 1.00 [Table 3]. The SEM values for all range of motion measurements were below or slightly above 2° as shown in [Table 3], except for two measurements. These two measurements were maximum angle and arc of motion for the activity of opening a tight jar, which had SEM of 8.7° and 8.8°, respectively. We note the thoracohumeral angles reported in [Table 3] differ slightly from the results in [Table 1]. [Table 3] shows thoracohumeral angle mean and standard deviations determined by both raters, whereas a single rater determined the thoracohumeral angles reported in [Table 1].
Table 2: Test-retest reliability for all subjects (n = 10)
Table 3: Inter-rater reliability and SEM for all subjects (n = 10)
Discussion
This study determined that shoulder flexion/extension during functional task performance could be assessed within 2° using video-based movement analysis and that approximately 120° of forward shoulder flexion/abduction, and 70° of shoulder extension are needed to perform five common tasks of daily life. The key findings include:
- Shoulder functional range of motion (ROM) identified in this study compared to similar studies;
- Healthy individuals require less than full shoulder range of motion (ROM) when performing five common ADL tasks;
- High participant variability was observed during performance of five ADL tasks; and
- Our motion analysis approach provides a clinically relevant tool to analyze shoulder function.
Shoulder ROM identified compares to similar studies
Although our approach differs from other studies [26],[27],[28] that compared shoulder ROM with PROMs, one previous study [28] also identified thoracohumeral angles in healthy subjects performing ADL activities using three-dimensional data from an electromagnetic tracking device. They identified that healthy individuals require approximately 120° of forward shoulder flexion, 45° of extension, and 130° of abduction to perform ADL tasks. Our findings are consistent with these results with respect to forward shoulder flexion; differences with respect to shoulder extension and abduction may be explained by variability in task performance as well, the approach used to assess movement (i.e., electromagnetic tracking device vs. video-based motion analysis). That we found similar functional ROM values using a video-based motion analysis software suggests that Dartfish provides a useful alternative to more complex movement analysis systems when assessing shoulder range of motion associated with functional tasks.
Healthy individuals require less than full shoulder range of motion (ROM) when performing five common ADL tasks
Five tasks were selected from the DASH items as they represent common functional tasks and because they are commonly assessed by self-report when the DASH is used as a PROM. Our motion analysis approach identified that these ADL tasks required 118°, 95% CIs (108, 128) of forward shoulder flexion, 112°, 95% CI (102, 120) of shoulder abduction, and −68°, 95% CI’s (−73, −62) of sagittal plane extension which is less than full shoulder ROM. These results are consistent with previous studies, [26],[27],[28] which also suggest that functional shoulder ROM to perform ADL tasks is less than full ROM. Furthermore, our study findings provide useful information for clinicians planning, implementing or evaluating surgical or rehabilitative interventions. For example, it can be difficult to determine whether the outcome is positive in some reconstructive “salvage” procedures [29] since “normal” function is not achievable. Evaluating the percentage functional ROM achieved can be a useful indicator of operative success when joint salvage procedures are performed.
High participant variability was observed during performance of five ADL task
This study demonstrated variable motion requirements of different functional tasks. The SEM for study measures was well within error margins that should be sufficient for clinical decision-making and efficiency of samples sizes within clinical trials. The low test-retest ICCs and high inter-rater ICCs are suggestive of individual variability during task performance that is also observed in high standard deviations. Since the movements were performed according to the participant preferences, we did not control how tasks were performed; thus, some variation in motion requirements is expected. Differences between participants in height, weight, and gender are also anticipated to have contributed to movement variability. Conversely, the measurement approach including marker placement, loss of marker visualization, and incorrect tracking of markers can contribute to measurement error. We expect these to be random measurement error (i.e., not biased); however, validation of Dartfish measures against traditional motion analysis systems is required to confirm this.
To reduce error, we used reflective markers and manual correction of tracking where these were poorly visualized and automatic tracking was lost. The measurements of maximum angle and arc of motion of ‘opening a tight jar’ had a lower ICC and a larger SEM compared to other measurements. The reasons for this are not clear although it was the only task where we provided any direction on task performance. Further, the variations in task performance were large, but the arc of motion was small, which means that errors were relatively larger. Overall, although we identified moderate test-retest reliability that we attribute to individual preferences during task performance, the inter-rater reliability for Dartfish showed excellent agreement suggesting that Dartfish provides a feasible alternative for identifying shoulder function that can be applied in clinical settings.
Our motion analysis approach provides a clinically relevant tool to analyze shoulder function
The observed participant variability during task performance has implications for functional expectations in different patient populations. For example, opening a heavy door or washing one’s back might be considered as having moderate shoulder movement demands since between 60° and 70° of flexion and 45° to 60° of abduction were required to perform these tasks. Generally, patients with rotator cuff disorders would not be expected to have this level of movement impairment. However, patients with total shoulder arthroplasty generally have more severe motion impairments. Hence, one might expect differences between these populations with respect to the percentage being able to perform these two functional tasks.
Furthermore, our study results have implications for the interpretation of the DASH. Opening a tight jar or heavy door required the least shoulder ROM with participants being able to perform this task with less than 25° of shoulder abduction. Moreover, patients may report little impact on this functional activity when shoulder motion is compromised. Consequently, specific items on the DASH or the shorter QuickDASH will be more salient to shoulder pathology noting that “open a tight jar” and “wash your back” are the two items from this study that were carried over to the QuickDASH. Using a video-based motion analysis approach such as Dartfish provides quantitative, biofeedback that can be used to identify differences between patient groups and identify functional requirements associated with PROMs. Furthermore, Dartfish provides a feasible alternative to traditional goniometric or other traditional approaches when providing immediate, relevant biofeedback to individuals with shoulder pathology in clinical settings.
Limitations
Movement analysis using this approach has some limitations. First, the shoulder joint marker was not placed at the center of joint rotation; therefore, joint angles were not measured by considering the center of rotation as the fulcrum. Thus, these angles may not represent true joint angles. However, placing markers on well-defined anatomical landmarks ensured reproducibility of the data as confirmed by the results of the rater reliability. The joint angles were calculated considering the acromion as the fulcrum of movement. A similar concept is used for standard goniometric ROM measurement of the shoulder joint, [22],[23] and subsequently, our data may be more clinically applicable as goniometric measures are traditionally measured in clinical settings.
We also observed that the tracking of the markers was dependent upon the quality of the video images. The quality of the video recorded by the standard definition camera was less optimal, and tracking was sometimes lost. Use of a high definition camera rectifies this limitation and is recommended in future applications of Dartfish movement analysis software. As well, when converting the motion data to a percent of task completion, we assumed participants performed tasks at constant velocity, which is a limitation of this approach.
Finally, our study participants were relatively young (29 ± 5 years) and had no shoulder pathology. The study outcomes may not apply to individuals outside of this age range; however, the primary objective of this study was to identify functional shoulder ROM requirements in healthy participants. The study findings provide information regarding functional shoulder movements required for ADL tasks that may be useful for clinicians when comparing functional outcomes post-surgery. In addition, the study findings will provide baseline and to inform future studies that might include patient perspectives.
Conclusions
Our study results suggest that healthy individuals require 118° of forward shoulder flexion, 112° of shoulder abduction and 68° of extension are needed to perform five ADL tasks, although high variability between participants was observed. Furthermore, our results suggest that Dartfish movement analysis software provides a reliable method for conducting a functional shoulder ROM assessment and may represent a viable quantitative clinical movement analysis tool for conducting functional ROM assessments. Future studies that incorporate Dartfish software are encouraged to consider the influence of both individual differences (i.e., gender, height, and weight) and shoulder pathology on shoulder movements during ADL task performance.